Revision rhinoplasty surgery presents some specific challenges to the plastic surgeon in addition to the inherent challenges of nose job surgery. Trauma of any kind, including surgical trauma, creates a degree of injury with resultant inflammation and tissue remodeling. Even after a precisely performed rhinoplasty surgery the healing process will create some degree of scar tissue, reshaping of the nasal skeleton – including the lower lateral cartilages comprising the tip, septum and middle vault.
Cartilage has resilience and flexibility, but scarring creates stiffness and inflexibility to the cartilage which makes subsequent reshaping even more challenging in the setting of a revision nose job surgery. In patients who have had multiple prior surgeries, the cartilage often contracts, often creating a foreshortened or upturned appearance to the nose. As a common goal for patients undergoing Asian rhinoplasty is to increase projection or augmentation of the nose, successful revision Asian nose job surgery must overcome this scar contracture. Special focus must be given to the rims of the ala and soft tissue facets in cases where the surgeon lengthens the nose or counter-rotates the infratip lobule. The rhinoplasty surgeon must perform appropriate structural grafting to the alar rims and transition into the infratip lobule to avoid issues with notching, alar retraction, and nostril asymmetry.
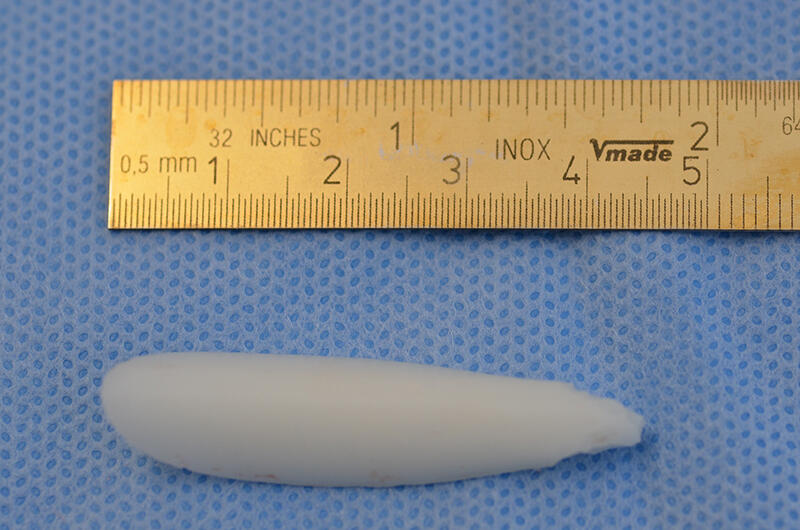
Placement of previous synthetic grafts, such as silicone, Goretex or Medpor, can also create a capsule of fibrosis and scar tissue within the nasal envelope. The presence of such a capsule can predispose the nose to develop contour irregularities or for poor fixation and positioning of a newly placed graft. Meticulous excision of previously placed alloplastic grafts and all resultant scar tissue will allow for more predictable healing of the nose after revision rhinoplasty surgery.
The baseline anatomy of most Asian noses differs from the typical anatomy present in the standard rhinoplasty operation during which a dorsal hump is reduced or a bulbous tip is narrowed, and thus the surgical techniques common to Asian nose job surgery differ quite a bit from the maneuvers performed in a reductive nose job. Given the contrasting challenges of primary Asian rhinoplasty vs. standard nose job surgery, revision Asian nose job surgery also poses special challenges for the Asian rhinoplasty surgeon to overcome.


