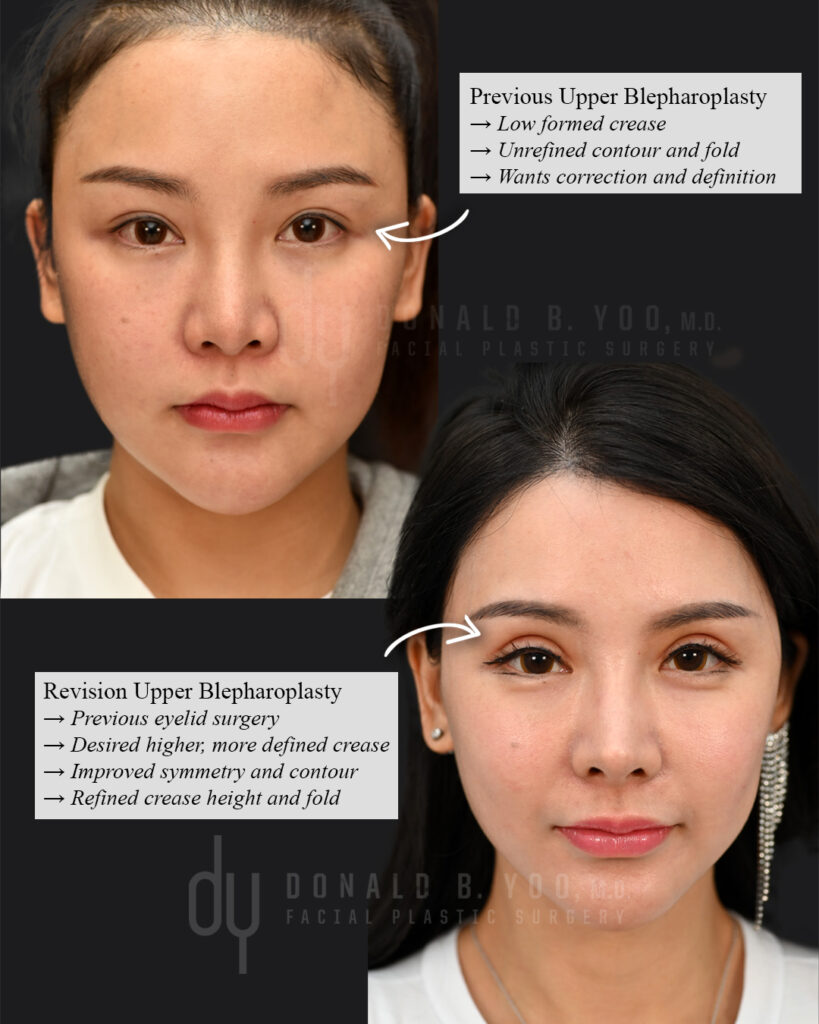
The periorbital area includes the upper eyelids and the eyebrows, and the interplay between the two anatomic units is important in creating a comprehensive rejuvenation to the eyes. For most patients the eyebrow position looks most aesthetically pleasing when the lateral aspect is level or slightly higher than the medial aspect, and the body of the eyebrow sits at or slightly above the supraorbital rim or brow bone. When the eyebrows are positioned higher than the brow bone it can lead to a startled or surprised appearance, while a position inferior or lower than the brow bone can contribute to an stern, angry or aged appearance. When the eyebrows are ptotic, the eyebrow skin may encroach on the upper eyelids or displace the upper eyelid skin inferiorly to create a hooded and heavy appearance to the upper eyelids.
When assessing the upper eyelids, the eyebrows must first be evaluated for their relative position. Once the normal position of the eyebrows has been established, then the surgeon may accurately assess the degree to which the upper eyelid skin is lax or redundant and can make a precise measurement in terms of the amount of skin removal. When the eyebrows are ptotic or droopy at their medial aspect, then an endoscopic browlift, direct browlift or coronal browlift may be indicated, depending on the patient’s anatomy and aesthetic goals. When the lateral brow is ptotic without accompanying ptosis of the medial brow, a temporal browlift may be most appropriate.
A temporal browlift involves incisions behind the temporal hairline bilaterally, and when executed precisely will not result in any change to the appearance of the hairline or alopecia. Within 3-6 months hair will typically grow through the incision and camouflage it completely. Through this hidden incision skin may be removed and dissection performed down to the orbital rim to release the connections tethering and pulling down on the brow. The same incision can be used to create further dissection into the midface and cheeks to perform and endoscopic facelift. In that instance suspension sutures are used to elevate the soft tissue and skin along the midface and, depending on the patient, the lateral canthus of the eyes, along with the brow/upper eyelid complex. In a temporal browlift the suspension sutures secure the mobilized skin/muscle/fascia flap to the deep temporalis fascia, creating a more open and refreshed appearance to the eyes. The elevation of the brows and brow skin allow for elevation of the supratarsal crease even when upper eyelid skin has not been surgically removed.